because writing 'write this in Management style nOTES'
was too long to write. In MGMT I had to write super detailed notes and it helped a lot. I want to do that more. here it is.
–Association cortex at the highest level, muscles at
the lowest
–Parallel structure – signals flow between levels
over multiple paths
•Motor output guided by sensory input
–Sensory feedback (all but ballistic - happen w/o mediation, swing bat etc )
•Learning (experience) changes the nature
and locus of sensorimotor control
–Conscious to automatic
starts @ association cortex down to smaller things
2 Major Areas of SensorimotorAssociation Cortex
•Each composed of several different areas with different functions • howdivide the areas up ?
•Posterior parietal association cortex (also for visual where pathway- good that they're connected so we can see where going)
•Integrates information about
–Body part location
–External objects
•Directs attention
•Receives visual, auditory, and
somatosensory information
•Outputs to motor cortex:
–Dorsolateral prefrontal association cortex,secondary motor cortex, frontal eye fields w/ damage in posterior parietal ass cortex
•Apraxia – disorder of voluntary movement
– problem only evident when instructed toperform an action – usually aconsequence of damage to the area onthe left - brush teetth in office no toothbrush
•Contralateral neglect – unable torespond to stimuli contralateral to the sideof the lesion - usually seen with largelesions on the right-
cooccurs w where they cant see things on left - cant move left arm etc
•Dorsolateral prefrontal association cortex(top sides of frontal)
•Input from posterior parietal cortex
•Output to secondary motor cortex, primarymotor cortex, and frontal eye field
•Evaluates external stimuli and initiatesvoluntary reactions – supported by neuronalresponses
•Strongest neuronal firing in anticipation of amovement
Secondary Motor Cortex
•Input mainly from association cortex
•Output mainly to primary motor cortex
•At least 7 different areas
–2 supplementary motor areas
•SMA and preSMA
SMA experiement - look at brain when moving spring, thinking about moving spring, and doing finger movement
–2 premotor areas
•dorsal and ventral
–3 cingulate motor areas
Subject of ongoing research
•May be involved in programming movements
in response to input from dorsolateral
prefrontal cortex
•Many premotor neurons are bimodal –
responding to 2 different types of stimuli
–E.g. visual and somatosensory
Primary Motor Cortex
•Precentral gyrus of the frontal lobe - does lots.
•Major point of convergence of corticalsensorimotor signals
•Major point of departure of signals from cortex
•Somatotopic – more cortex devoted to body parts which make many movements
•Control of hands involves a network of widelydistributed neurons - move one part of hand, effect all hand neurons
–Focal Dystonia - when some fingers are so interelated that you forget that they are seperate entities - pinky and ring move a lot w/ middle finger - so middle finger moves and ring and pinky move with it. happens in pianists.
•Stereognosis – recognizing by touch –requires interplay of sensory and motorsystems
•Some neurons are direction specific – firingmaximally when movement is made in onedirection
4:40
subcortical you ask?
Cerebellum and Basal Ganglia
•Interact with different levels of thesensorimotor hierarchy
•Coordinate and modulate
•May permit maintenance of visuallyguided responses despite corticaldamage
Cerebellum
10% of brain mass but has 50% of neurons in brain
•Input from 1° and 2° motor cortex
•Input from brain stem motor nuclei
•Feedback from motor responses
•Involved in fine-tuning and motor learning
–Learning of sequences or movements wheretiming is critical
•Up with the cerebellum, down with the frontal lobes! - we do better if we dont think about it. want it to be automatic.
–Damage - problems with direction, force, velocity& amplitude of movements, adapting, posture,balance, gait, speech, eye movements
•May also do the same for cognitive responses
- help coordinate to changing stimuli
Basal Ganglia
•A collection of nuclei
•Part of neural loops that receivecortical input and send output back via the thalamus
•Modulate motor output and cognitivefunctions
–Response learning - learned associations
•Abnormal functioning involved in Tourette’ssyndrome (as)- smoothness of movement -
•Substantia Nigra–Loss of nerve cells causes Parkinson’s disease - hyperkenesia - cant stop moving - diskenisia - cant movie. --- cerebellum just working - when he ice skates - no symptoms- video of micheal j fox
•2 ventromedial - figure 8.8- take over motor movements if dorso thing fails- but cant do just reaching single limbs out.
–Corticospinal
–Descends ipsilaterally
–Axons branch and innervate interneuron circuits bilaterally
in multiple spinal segments
–Cortico-brainstem-spinal tract
–Interacts with various brain stem structures and descends
bilaterally carrying information from both hemispheres
–Synapse on interneurons of multiple spinal segments
controlling proximal trunk and limb muscles
Ventromedial
•Both corticospinal tracts are direct
•one direct tract, onethat synapses in thebrain stem•More diffuse•Bilateral innervation•Proximal muscles •Posture and wholebody movement
Motor Units and Muscles
•Motor units – a motor neuron + muscle
fibers, all fibers contract when motorneuron fires (contraction message)
•Number of fibers per unit varies – finecontrol(1-1 ratio), fewer fibers/neuron
•Muscle – muscle fibers bound togetherby a tendon
•Acetylcholine (curare and botox are antagonists of acetyocholine) released by motor neurons at theneuromuscular junction causes contraction
•Motor pool – all motor neurons innervating the fibersof a single muscle
•Fast muscle fibers – fatigue quickly - they work quickly when you need rxn but they dont have a great supply of oxygen or blood - sprinting
•Slow muscle fibers – capable of sustainedcontraction due to vascularization - capable of sustained contraction - swimming vs running - have good blood and oxy flow
• all Muscles are a mix of slow and fast
•Flexors – bend or flex a joint
•Extensors – straighten or extend
•Synergistic muscles – any 2 muscleswhose contraction produces the samemovement
•Antagonistic muscles – any 2muscles that act in opposition
•Reciprocal innervation – antagonistic(that do opp move w/ joint) muscles interact so that movementsare smooth – flexors are excited whileextensors are inhibited, etc.-
Recurrent collateral inhibition - each timea motor neuron fires, it momentarilyinhibits itself via Renshaw cells- cant fire twice real quick - so it doesnt hurt itself - take turns
back to more general...
Central SensorimotorPrograms
•Perhaps all but the highest levels of thesensorimotor system have patterns of
activity programmed into them andcomplex movements are produced byactivating these programs
•Cerebellum and basal ganglia thenserve to coordinate the variousprograms
Motor equivalence
•A given movement can be accomplishedvarious ways, using different muscles
•Central sensorimotor programs must bestored at a level higher than the muscle (asdifferent muscles can do the same task)
•Sensorimotor programs may be stored insecondary motor cortex
–Signing name
The Development of CentralSensorimotor Programs
•Perception & sensorimotor programs (figure 8.17 - the moon! )
•Programs for many species-specific
behaviors established without practice
–Fentress (1973) – mice without forelimbs stillmake coordinated grooming motions
•Practice can also generate and modifyprograms
–Response chunking–Practice combines the central programscontrolling individual response•E.g. typing (hunt and peck v touch typing )
–Shifting control to lower levels–Frees up higher levels to do more complextasks–Permits greater speed
Motor cortex-controlled robots- vid
Summary
•The motor cortex is organized much like thesensorimotor cortex, information just flows inthe opposite direction.
•The brain strives to perfect movementsthrough feedback and move them from upperto lower levels.
•Movement can happen at the level of themotor unit, usually to enhance survival.
test on tuesday - read 5, 6, skim 7. read 8, take notes.
journal entry - a patient comes to the dr complaining that his body doesnt move like it used to. the joints have been ground down so bones are rubbing together and wearing away - he doesnt have a physically intense job - - the dr figures it out as soon as she sticks patient w/ needle - what sense is this patient missing
he can't feel pain
nociceptive - can't feel pain from outside
interoceptive - can't feel pain from inside.
sensory areas of the cortex
primary sensory cortext - direct input mainly from thalamix relaty nuclei
ie striate cortex recives input from LGN
secondary sensory contex - inpyt from pri and sex cortex w/in sensory system
association cortex - input from more than one sensory system - usually from 2nd sens system
principles guiding sensory cortex interactions
heirarchal org.
specificity and complexity increases w/ each level.
sensation - detect a stimluus
perception - understanding stimulus
functional segregation
color/movement have own modules
parallel processing - like computers - do it faster
Sensory system organization
picture - in book figure 7.2
multiple specialized areas @ multiple levels, interconnected by many parallel pathways
the binding problem - how does brain finally integrate info- but there are corticofugal pathways that allow higher areas to influence lower areas - higher being cortex, lower being subcortical
Visual cortex
Primary (v1) - posterior occiptal lobe
secondary
prestriate cortex - band of tissue around v1
inferotemporal cortex
Association - various areas, largest single areas is in posterior parietal cortex
bc we have parallel network - if one thing breaks, it will still work around it.
study of Scotomas - area of blindness resulting from V1 damage
hemianopsic - last perception in half of visual field
blind in corresponding contralateral visual field of both eyes
deficit may or may not be readily detected bc of completion (like blond sport)
seeing stars is a temporary scotomas
Blindsight
ability to respond to visual stimulus even w no conscious awareness of the stimulus
putting coins in slot - they can do it even if they cant see it
may still be connections in v1 allowing for reactions w/p awareness
may be that message gets to brain by connections that dont pass thru scotoma.
-video about blindsight patient who cant see - but can process stuff - cool. - kirsten - ask me and i'll explain it better - about movement
"vision is not entirely seeing there can be a something to respond to visual info and being able to see"- messed up quote :)
notes continued
without this zombie in our brain helping us have autopilot - like driving
grahm's blindness - cant see, but can sense- perception w/o sensation/conciousness- like video
like subjective contours - white triangle, cube, pyramid - figure 7.6
dorsal and ventral streams
dorsal stream - where - /control of behavior
v1 to dorsal prestriate to posterior parietal
ventral stream - what - /conscious perception
v1 to ventral prestriate to inferotemporal
both where and what ///behavior/percetion distinctions are supported by effects of damage
not so much kinds of info - but the use to which that info is put - do we use it to interact w/ objects or see them or what
photo - figure 7.9
theres lots of types of chairs - so object recog just tells us - yes this is a chair
Aperceptive agnosia - difficulty in perceiving basic elements that make up an object - dependent on amount and location of damage- cant percieve X to cant perceive complex
cant copy pictures - like stick drawings
Associative Agnosia
- difficulty in assigning meaning to an object it cant be recognized
can copy pictures
cant build whole representation for object
cant get generalize categories sometimes
the man who mistook his wife for a hat
Prosopagnosia - cant recog faces agnosia for faces
can say this is a face - but not bc
damage to hippocampal formation
also have trouble saying which cow or which chair
can be damage to ventral/what stream
thus unconscious recog can be hypothesized
has been supported - altered auto responses.
fusiform face area- activity increased during face recog but not recog for other objects
areas in ventral stream may be specific to humans, cats , houses, other broad categories
each area responds to each class but there is a great overlap in areas.
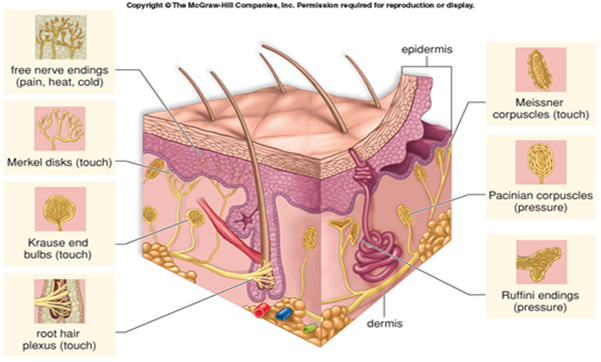
exteroreceptive- touch(mech stimuli), temperature (thermal), pain (nociceptive)
Cutaneous receptors
free nerve endings , temp and pain
Pacinian copuscles (shapes like onions)
adapt rapidly, large and deep
sudden displacements of skin
Merkel's disks - gradual skin indentation
photo : ruffini ending merkels disks etc
respond to ∆
stereognosis - identify objects by touch
dermatome - area of body innrvated by left and right dorsal roots of a given segment of a spinal cord -figure 7.16
ascending somotosensory pathways
dorsal columbn medial lemniscus system
touch and prprioception
1st synapse in dorsal colum nuclei of the medula
anterolateral system
pain and temp
synapse upon enter spinal cord
Primary Somatosensory cortex (SI)
postcentral gyrus
somatotopic
more sens = more cortex
input mostly contralateral
SII mainly imput from SI
somatopic - imput from both sides of body
somatosensory homonuculus
receptive fields
- can be divided to excitatory and inhibitory areas
-rubbing a bite or owwie makes pain get less - by rubbing you stimulate other nerve endings and causes lateral inhibition of pain things - makes you feel contact and not pain
Asterogognosia - inability to recog objects by touch
Asomatognosia - failure to recog parts of own body - aunt betty/man who fell out of bed
Anosgnosia - hmm, i missed this one. i think its thinking your foot is there when its been amputated.
paradoxes of pain
- despite unpleasantness, pain is adaptive and needed
- existences of endogenous (we make them, occurs w/in) opiates - natural analgesics - they are endorphins
Chemical senses
olfaction - smell--phermones (early research, not proven)- 1000s of receptors , they regenerate. figure 7.23
gustation - taste-- receptors in tongue and oral cavity - clusters of 50 called taste buds. >4 -sweet sour salty bitter - primary tasted - 5th is unami - meat or savory - many tastes are not created by combining primaries
food acts on both systems to produce flava
Brain damage and chem senses
- Anosmia - inability to smell
most common cause = blow to head that damages olfactory nerves
incomplete deficts seen w. variety of disorders
-Ageusia - inabilty to taste
rare bc we use 3 nerves to taste - so we'd have to damage all.